Ever looked at a brain scan and felt like you were staring at a Rorschach test? You're not alone. When a doctor orders a Brain MRI is a non-invasive diagnostic technique that uses powerful magnetic fields and radio waves to create detailed images of the brain, it's usually because they need a level of detail that a standard CT scan just can't provide. While the images look like grey-and-white swirls to the untrained eye, they contain a map of your neurological health, showing everything from the flow of fluid to the integrity of your white matter.
If you've just received a report or are preparing for a scan, the first thing to understand is that an MRI isn't just one picture. It's a collection of different "sequences." Think of these like different filters on a camera; one filter might highlight water, while another makes fat pop. By switching these filters, radiologists can spot a tiny stroke or a hidden tumor that would otherwise blend into the background.
The Key MRI Sequences and What They Actually Show
To make sense of a brain scan, you have to know which "filter" the radiologist is using. Each sequence highlights a different attribute of the brain tissue. Here is the breakdown of the ones you'll see most often in a clinical report.
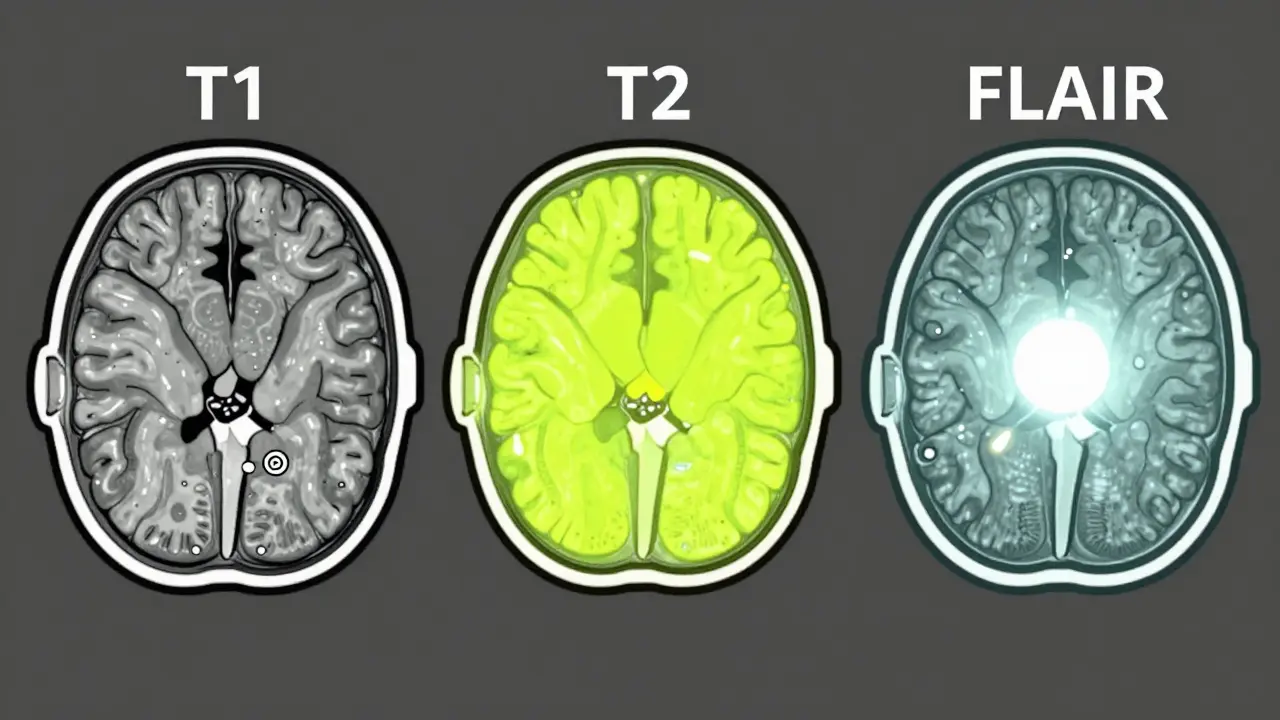
- T1-weighted imaging: This is the "anatomy scan." In T1, fat looks bright and cerebrospinal fluid (CSF) looks dark. It's the best way to see the physical structure of the brain and where things are located.
- T2-weighted imaging: This is the "pathology scan." Here, water and fluid look bright. Since most brain injuries, tumors, and inflammation involve swelling (edema), T2 makes these problems glow, though it can be hard to tell a lesion from normal brain fluid.
- FLAIR: Short for Fluid-Attenuated Inversion Recovery. This is a modified T2 scan that "turns off" the signal from normal fluid. If something stays bright on a FLAIR image, it's usually a sign of a lesion, which is why it's the gold standard for spotting multiple sclerosis plaques.
- Diffusion-Weighted Imaging (DWI): This is the emergency tool. It detects how water molecules move. In an acute stroke, water gets trapped, creating a bright signal. DWI can spot an ischemic stroke within minutes, whereas other scans might take hours to show anything.
- SWI: Susceptibility-Weighted Imaging is specifically designed to find blood. It picks up tiny deposits of iron (hemosiderin) from old bleeds, making it incredibly sensitive to microhemorrhages.
| Sequence | What looks bright? | Primary Use | Key Strength |
|---|---|---|---|
| T1 | Fat / Contrast | Anatomy | Clear structural boundaries |
| T2 | Water / Fluid | Identifying Lesions | High sensitivity to edema |
| FLAIR | Pathological Fluid | MS / Inflammation | Removes normal fluid "noise" |
| DWI | Restricted Water | Acute Stroke | Immediate detection of infarction |
| SWI | Blood / Iron | Hemorrhage | Spots tiny microbleeds |
Why Choose MRI Over a CT Scan?
You might wonder why you can't just get a quick CT scan. The truth is, for most neurological issues, MRI is simply superior. While a CT scan is great for a quick look at a bone fracture or a massive bleed in an ER setting, it lacks the resolution to see the "soft stuff." MRI provides about 100 times better contrast for differentiating between gray and white matter.
One specific area where MRI wins is the posterior fossa (the back of the brain). CT scans often struggle here because the thick skull bone creates "beam-hardening artifacts"-basically, shadows that hide potential tumors or strokes. MRI doesn't have this problem. Furthermore, if you need repeated scans to monitor a chronic condition, MRI is the only safe choice because it doesn't use ionizing radiation.
However, MRI isn't always the answer. It takes much longer-usually 30 to 45 minutes compared to the 5 minutes for a CT. If a patient is unstable or in critical condition after a trauma, a CT is the way to go. Plus, the magnetic field means anyone with certain metallic implants, like older pacemakers or cochlear implants, might not be able to enter the machine.
Decoding Common Findings in the Report
When you read your radiology report, you'll see terms that sound scary but are often quite common. For instance, you might see mentions of "hyperintensities." In plain English, a hyperintensity is just a spot that looks brighter than the surrounding tissue on a T2 or FLAIR scan. Does this always mean a disease? Not necessarily.
About 90% of people over 70 have some periventricular hyperintensities-small bright spots around the fluid-filled spaces of the brain. In many cases, these are just signs of aging or small vascular changes. The key is the location. If those spots are in specific areas, like the temporal lobes, it might suggest an infection like herpes encephalitis. If they are concentrated in the parietal-occipital regions, it could point toward a specific syndrome related to blood pressure spikes.
Another common finding is "atrophy," which is the shrinking of brain tissue. Experienced radiologists look at this on FLAIR images specifically. If they used T2 images, the bright cerebrospinal fluid can make the ventricles (the brain's fluid cavities) look larger than they actually are, which might lead to an overestimation of how much the brain has shrunk.
How Radiologists Actually Read Your Scan
Reading a brain MRI isn't about glancing at a picture and guessing. It's a systematic process. A radiologist typically starts at the midline and works their way out. They'll check the ventricles first, then move to the subcortical structures, the lobes, the cortex, and finally the skull and meninges.
They are also hunting for "incidentalomas"-findings that aren't related to why you got the scan but are still important. For example, a radiologist will always check the cerebellopontine angle. Why? Because that's where small acoustic neuromas (benign tumors on the hearing nerve) hide. MRI can detect these when they are as small as 2mm, often before the patient even notices any hearing loss.
Another focus area is the basal ganglia and thalamus. Radiologists look for tiny bright spots here that indicate "lacunar infarctions." These are essentially tiny, silent strokes that didn't cause a major event but tell the doctor a lot about the patient's long-term vascular health.

The Future of Neuroimaging
We are moving beyond just "looking" at images toward "measuring" them. While 1.5T and 3.0T magnets are the current standard, ultra-high field 7.0T MRI systems are now being used in academic centers. These machines provide such incredible resolution (down to 0.5mm) that doctors can actually see the individual layers of the cerebral cortex.
Artificial Intelligence is also changing the game. New software can now reduce scan times by up to 50% without losing any detail, which is a huge win for patients who struggle with claustrophobia. We're also seeing the rise of DTI (Diffusion Tensor Imaging), which allows doctors to map the white matter tracts-the "wiring" of the brain-to see exactly how different regions are communicating.
Is a brain MRI safe for everyone?
Most people can safely undergo an MRI, but it is not for everyone. Because the machine uses a powerful magnet, people with ferromagnetic implants-such as certain pacemakers, cochlear implants, or certain types of aneurysm clips-cannot have an MRI. Always disclose all surgical implants to your technician.
Why does my report mention "hyperintensities" if I feel fine?
Hyperintensities are simply areas that appear brighter than usual on specific MRI sequences. While they can indicate things like MS plaques or old strokes, they are also very common as a natural part of aging. In people over 70, up to 90% show some level of periventricular hyperintensity without having a significant neurological disease.
How long does a typical brain MRI take?
A standard clinical brain MRI usually takes between 30 and 45 minutes. This time is necessary to run multiple different sequences (like T1, T2, and FLAIR) to get a complete picture of the brain's health.
What is the difference between an MRI and a CT scan?
A CT scan uses X-rays and is very fast, making it ideal for bone fractures and acute trauma. An MRI uses magnetic fields and is much slower but provides far superior detail of soft tissues, making it the gold standard for diagnosing most central nervous system diseases.
Does an MRI use radiation?
No, brain MRI does not use ionizing radiation. This makes it much safer for children and for patients who require frequent monitoring of a chronic condition over many years.
Next Steps After Your Scan
If you've just had your results come back, the best thing you can do is prepare a list of questions for your neurologist. Don't just ask "is it normal?" Instead, ask: "Are these findings typical for my age?" or "Do these hyperintensities correlate with my specific symptoms?"
If your report suggests "nonspecific findings," don't panic. This often means the radiologist sees something that doesn't fit a clear pattern of disease and requires a clinical correlation-meaning your doctor needs to match the image with your actual physical symptoms to make a diagnosis.




Comments
Robin Walton
April 10, 2026 AT 15:55 PMThis is actually super helpful for anyone currently freaking out over a radiology report. Those terms can be so intimidating when you first see them on a screen.
Rakesh Tiwari
April 11, 2026 AT 07:25 AMOh wow, imagine thinking a simple guide like this is enough to replace an actual medical degree. How charmingly naive of some people to think they can just skim a blog post and suddenly understand the complexities of neuroimaging. Truly a triumph of modern confidence over actual competence.
Julie Bella
April 12, 2026 AT 11:36 AMOmg i just had one of these last month and the noise was so loud!! 😱 i totally agree with the part about anxiety. does any1 else feel like the techs dont explain enough?? i bet some of u guys have had bad experiences too!! tell me everything!! ✨
Will Gray
April 12, 2026 AT 19:23 PMThe push for 7.0T machines is just a front for more intrusive surveillance. While the plebeians cheer for 'resolution,' the elite are just finding new ways to map our thoughts. It is a disgrace that only the most advanced centers in the West have this, as if the globalists aren't already using it to curate who gets the 'best' care based on loyalty to the state.
Franklin Anthony
April 13, 2026 AT 09:13 AMits funny how they talk about ai making scans faster but they dont mention who owns the data the ai is training on probably some big corp selling your brain maps to insurance companies lol just a little food for thought while you lay in that tube
Victor Parker
April 14, 2026 AT 00:08 AMBig Pharma and the MRI industry are just keeping us in a loop of 'monitoring' so they can sell more drugs for those 'hyperintensities' they suddenly found 🙄 just try some natural detox and you wont need a 3.0T magnet to tell you your brain is shrinking 🌀
Emily Wheeler
April 15, 2026 AT 20:25 PMThe intersection of technology and human consciousness is such a fascinating realm to explore, and while the technical aspects of T1 and T2 sequences are undeniably impressive from a clinical standpoint, I find myself wondering if the sheer precision of these images actually enhances our holistic understanding of the patient's lived experience or if it simply reduces a complex human soul into a series of high-contrast voxels and algorithmic patterns, though we must remain optimistic that this progress will eventually lead to a more compassionate form of medicine that blends the quantitative data of a FLAIR scan with the qualitative reality of human suffering.
Peter Meyerssen
April 16, 2026 AT 10:25 AMThe ontological implications of DTI are simply transcendent 🌌. We are basically talking about the phenomenology of the connectome, where the structural anisotropy becomes a metaphor for the human condition. Totally peak science, but honestly, the jargon in these reports is just a linguistic barrier to gatekeep the transcendental nature of our grey matter. 💅
Ryan Hogg
April 16, 2026 AT 19:06 PMI had one of these for my chronic migraines and the waiting for the results was the worst part of my entire year. I couldn't sleep for three days because every time I closed my eyes I just saw that T2 image in my head and I was convinced I had a tumor and nobody cared that I was spiraling. It's just so draining when the doctors use words like 'nonspecific' because it feels like they're just dismissing the pain I feel every single day while they stare at a screen.
danny Gaming
April 17, 2026 AT 07:47 AMCT is just way fastr for real and most of these mri things are overkill for basic checks probly just a way to charge more for the insurance’s sake lol i bet the US systems are the only ones actually making money off this garbage