
Metformin Alcohol Risk Calculator
Personal Risk Assessment Tool
This tool estimates your risk of metformin-associated lactic acidosis (MALA) based on your drinking habits and health factors. Note: This is for informational purposes only. Always consult your healthcare provider for personalized medical advice.
Key Takeaways
- Metformin combined with heavy alcohol use can trigger metformin‑associated lactic acidosis (MALA), a life‑threatening condition.
- The overall incidence of MALA is under 0.03 per 1,000 patient‑years, but binge drinking can raise that risk markedly.
- Renal impairment, acute alcohol intoxication, and chronic heavy drinking are the strongest risk drivers.
- Moderate drinking (<=1 drink/day for women, <=2 for men) may be acceptable for patients with normal kidney function, but no clinical threshold is officially established.
- Early symptoms mimic a hangover; immediate medical evaluation is crucial if they appear.
When you hear people talk about Metformin and alcohol, the first thing that should pop into your head is safety. The combination isn’t a recipe for a bad night‑out; it can spark a rare but deadly metabolic disaster called metformin‑associated lactic acidosis (MALA). Below we unpack how the two substances interact, who should worry most, and what you can do right now to stay safe.
Metformin is a biguanide oral antihyperglycemic agent that lowers blood glucose by inhibiting hepatic gluconeogenesis. First approved by the U.S. FDA in 1995 under the brand name Glucophage, it is the world’s most prescribed first‑line therapy for type 2 diabetes.
What Is Metformin and Why Is It So Popular?
Metformin works mainly in the liver, where it blocks the production of new glucose. By doing so, it reduces the amount of sugar released into the bloodstream, helping fasting glucose and HbA1c levels drop. Its benefits extend beyond glucose control: it modestly improves lipid profiles, may aid modest weight loss, and carries a very low risk of causing low blood sugar (hypoglycemia) when used alone.
Because of its safety, affordability, and decades of real‑world data, major guidelines-from the American Diabetes Association (ADA) to the European Association for the Study of Diabetes (EASD)-recommend metformin as the first medication after lifestyle changes.
How Alcohol Messes With Metformin’s Metabolism
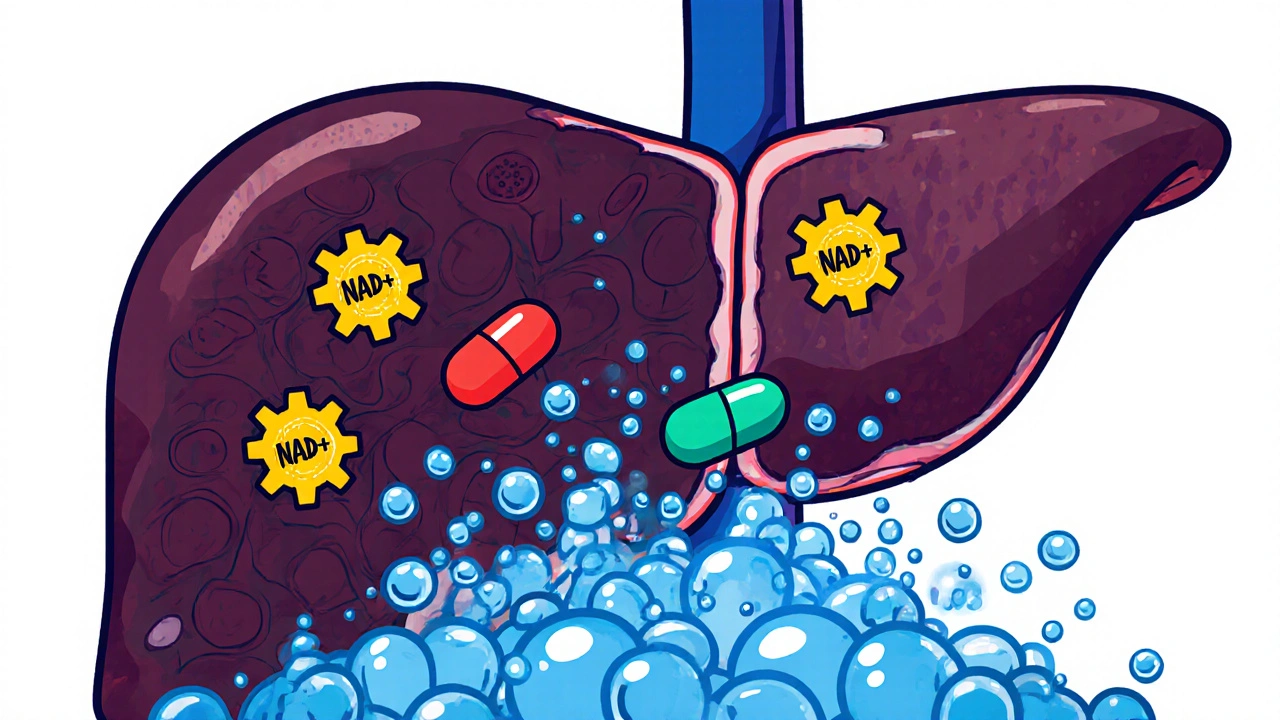
Alcohol is broken down in the liver by alcohol dehydrogenase, a process that consumes nicotinamide adenine dinucleotide (NAD+). When NAD+ is tied up converting ethanol to acetaldehyde, the liver’s ability to convert lactate back into glucose (the Cori cycle) stalls. In parallel, metformin already nudges the liver toward more lactate production by suppressing gluconeogenesis. Put the two together, and you get a double hit: more lactate enters the bloodstream while the liver’s clearance capacity shrinks.
Most of metformin is eliminated unchanged by the kidneys-about 90 % of a dose is cleared through renal filtration. Alcohol can also cause a temporary dip in urine output and blunt renal perfusion, further slowing metformin excretion. The result is higher circulating metformin levels, which, when combined with reduced lactate clearance, set the stage for MALA.
Understanding Lactic Acidosis
Lactic acidosis is defined by a blood lactate concentration >5 mmol/L and a pH < 7.35, often accompanied by an anion‑gap increase. In the context of metformin, clinicians look for plasma metformin levels >5 µg/mL, although many cases present with normal drug levels if the kidneys are still working.
Symptoms are non‑specific and can be mistaken for a severe hangover:
- Unexplained muscle cramps or weakness
- Rapid breathing (hyperventilation) to compensate for metabolic acidosis
- Nausea, vomiting, and abdominal discomfort
- Generalized fatigue and dizziness
Because these signs overlap with intoxication, patients often delay seeking care, which increases mortality. Reported case‑fatality rates range from 30 % to 50 %.
Who’s at Higher Risk?
Risk isn’t spread evenly across every metformin user. The biggest red flags are:
- Renal impairment: eGFR < 45 mL/min/1.73 m² dramatically raises metformin accumulation risk.
- Acute alcohol intoxication: binge drinking (≥4 drinks for women, ≥5 for men within 2 hours) spikes lactate production.
- Chronic heavy drinking: regular intake >14 drinks/week for men or >7 for women depletes NAD+ stores.
- Concurrent hepatotoxic drugs or conditions that already impair lactate clearance (e.g., sepsis, heart failure).
Even patients with perfectly normal kidneys can develop MALA if they combine metformin with severe binge drinking, as documented in a 2024 case study of a 65‑year‑old man with type 2 diabetes who presented with a lactate of 6.2 mmol/L after a night of heavy beer consumption.
Is Metformin the Only Diabetes Drug That Worries About Lactic Acidosis?
Compared to older biguanides-most notably phenformin, which was pulled from the market in 1978 after a 40‑64 % lactic acidosis incidence-metformin’s risk is tiny (≈0.03 per 1,000 patient‑years). Other oral agents don’t share this danger:
- Sulfonylureas can cause hypoglycemia but not lactic acidosis.
- DPP‑4 inhibitors and GLP‑1 receptor agonists are mainly linked to gastrointestinal upset or pancreatitis.
- SGLT2 inhibitors raise the risk of urinary tract infections and rare euglycemic ketoacidosis.
Nevertheless, the FDA’s black‑box warning for metformin still calls out “excessive alcohol intake” as a special precaution, while newer agents only mention generic alcohol warnings.
Comparison of Lactic Acidosis Risk Across Common Diabetes Medications
| Medication | Incidence | Alcohol Interaction | Key Contra‑indication |
|---|---|---|---|
| Metformin | 0.3 | Increases risk, especially with binge drinking | Renal impairment, acute metabolic acidosis |
| Phenformin (withdrawn) | 35‑64 | High‑risk, no safe alcohol level | Renal failure, liver disease |
| Sulfonylureas | <0.1 | No direct effect | Hypoglycemia risk |
| DPP‑4 inhibitors | <0.1 | No direct effect | Pancreatitis (rare) |
| SGLT2 inhibitors | <0.1 | No direct effect | Euglycemic ketoacidosis |
Practical Guidance for Patients on Metformin
Because the science hasn’t nailed a “safe” alcohol limit for metformin users, clinicians rely on common‑sense rules. Here’s a checklist you can keep on your phone or fridge:
- First 4‑8 weeks: avoid alcohol completely while you’re still titrating the dose.
- After stabilization: if you have normal kidney function (eGFR ≥ 60), many doctors advise staying within moderate‑drinking guidelines-no more than 1 drink per day for women, 2 for men.
- Never drink on an empty stomach while taking metformin, as this can worsen nausea and hypoglycemia.
- Watch for early warning signs-muscle pain, rapid breathing, abdominal pain, or unexplained fatigue-and seek care immediately.
- Stay hydrated and consider spacing your dose (e.g., take metformin with food).
- Check kidney function annually; if eGFR drops below 45, discuss dose reduction or an alternative medication with your doctor.
What to Do If You Suspect Lactic Acidosis
Time is the biggest factor. If you notice any of the red‑flag symptoms, follow these steps:
- Call emergency services (999 in the UK, 911 in the US) and tell them you’re on metformin and have been drinking.
- Do not wait for the symptoms to “pass” like a regular hangover; ask for immediate blood gas and lactate testing.
- If you’re at a hospital, the treatment usually involves IV bicarbonate, aggressive hydration, and possibly dialysis to clear metformin.
- After discharge, schedule a follow‑up with your endocrinologist to reassess medication choice.
Future Directions: Research and New Formulations
New extended‑release (ER) metformin tablets entered the U.S. market in 2023. They spread the drug’s absorption over a longer period, which helps stomach upset but does not change the lactic‑acidosis warning. Ongoing trials-like the MALA‑Prevention Study (NCT04892345) launching in early 2024-aim to pinpoint exact alcohol thresholds that raise risk. Preliminary data expected in late 2025 may give clinicians clearer guidance than the current “avoid excessive alcohol” phrase.
Meanwhile, some researchers are exploring alternative pathways, such as adding NAD+ precursors (e.g., nicotinamide riboside) to offset the NAD+ drain from alcohol metabolism, but these are still in early phases.
Bottom Line
If you take metformin, treat alcohol like a strong medication: enjoy it sparingly, never binge, and always stay alert for the subtle signs of lactic acidosis. The risk is low for most patients, but the consequences can be severe, so a little caution goes a long way.
Can I have a glass of wine with dinner while on metformin?
Moderate intake (up to one glass for women, two for men) is generally considered acceptable if you have normal kidney function and avoid binge drinking. However, no official safe limit has been proven, so discuss your habits with your doctor.
What are the early symptoms of metformin‑associated lactic acidosis?
Look for unusual muscle cramps, rapid breathing, nausea, abdominal pain, or a sudden feeling of extreme fatigue that doesn’t improve with rest. These can be mistaken for a hangover, so seek medical help right away.
Does the type of metformin (immediate‑release vs. extended‑release) affect the risk?
Both formulations carry the same black‑box warning for lactic acidosis. The ER version may cause fewer gastrointestinal side effects but does not change how the drug is cleared or its interaction with alcohol.
Should I stop metformin if I’m planning to drink heavily at a special event?
Yes. If you anticipate binge drinking, it’s safest to pause metformin for at least 48 hours and resume only after normal kidney function is confirmed, or switch to an alternative diabetes medication for that period.
How does chronic alcohol use affect my B12 levels while on metformin?
Both metformin and alcohol can lower vitamin B12 absorption. Over time, you may develop deficiency, leading to neuropathy. Regular B12 screening every 1‑2 years is advised, with supplementation if levels drop.




Comments
Ramesh Kumar
October 26, 2025 AT 19:20 PMHey there! If you're on metformin and enjoy the occasional drink, the key is moderation and kidney health. Your kidneys clear metformin, so an eGFR above 60 mL/min usually keeps drug levels safe. Binge drinking, however, spikes lactate production and can push you into MALA even with normal kidneys. Stay hydrated, never drink on an empty stomach, and watch for rapid breathing or unexplained muscle cramps – those are red flags. Talk to your doctor about your drinking patterns during your next check‑up.
ahmed ali
October 28, 2025 AT 13:49 PMLook, i gotta be honest, i think the whole panic about metformin + booze is kinda overblown, especially when you read the actual stats – under 0.03 cases per 1,000 patient‑years is practically nothing, ya know? Most folks who binge drink already have other health issues that would kill them faster than a little lactic acidosis, so blaming the pill is just a convenient scapegoat. Plus, the studies that link binge drinking to MALA often have tiny sample sizes and vague definitions of “heavy” alcohol use, which makes the conclusions kinda shaky. If you’re worried, just stick to the standard “one‑drink‑a‑day” rule, and you’ll be fine – no need to live in fear of a phantom hangover. Also, the newer extended‑release metformin has a smoother absorption curve, which i’m pretty sure reduces the lactate spike, even though the FDA hasn’t updated the warning yet. Don’t forget that other meds like SGLT2 inhibitors can cause euglycemic ketoacidosis, which is actually rarer but arguably more dangerous. So yeah, keep your eyes on the bigger picture, don’t let a single black‑box warning run your whole life. Finally, if you ever feel weird after a night out, get checked – but don’t assume metformin is the villain until you’ve ruled out infections or heart issues.
Deanna Williamson
October 30, 2025 AT 08:18 AMYour friendly advice sounds nice, but it glosses over the biochemical reality: alcohol metabolism consumes NAD+, which directly hampers lactate clearance independent of metformin levels. The interaction isn’t just “drink on a full stomach”; it’s a mechanistic synergy that can push lactate from 2 to 6 mmol/L in minutes. Moreover, the data you cite about eGFR thresholds are derived from heterogeneous cohorts, making the “safe above 60” claim questionable. Clinicians should be wary of generalized statements and instead assess individual hepatic and renal reserve before giving blanket permissions. Ignoring these nuances risks under‑informing patients about a potentially fatal event.
Miracle Zona Ikhlas
November 1, 2025 AT 02:47 AMGreat summary – staying within moderate limits and monitoring kidney function is the safest path.
naoki doe
November 2, 2025 AT 21:15 PMHonestly, I’ve seen too many people treat the warning like a polite suggestion when it’s actually a life‑or‑death clause. If you’ve ever mixed metformin with a weekend binge, you probably know the after‑effects better than any article. Just remember: skipping your dose before a party isn’t cheating, it’s smart.
Joe Langner
November 4, 2025 AT 15:44 PMThats why i always keep a water bottle handy.
Katherine Brown
November 6, 2025 AT 10:13 AMIn accordance with the current clinical guidelines, patients with an estimated glomerular filtration rate (eGFR) of less than 45 mL/min/1.73 m² should avoid metformin entirely, irrespective of alcohol consumption. For individuals whose eGFR lies between 45 and 60 mL/min/1.73 m², clinicians are advised to limit the dosage and counsel on strict moderation of alcohol intake. Annual monitoring of renal function and lactate levels is prudent, particularly after any episode of acute intoxication.
Charlene Gabriel
November 8, 2025 AT 04:42 AMReading through all these points really underscores how much we can empower ourselves with knowledge. First, understanding that metformin is a cornerstone of type‑2 diabetes management helps us appreciate why we don’t want to toss it away without good reason.
Second, recognizing that alcohol is a double‑edged sword – enjoyable in moderation but potentially hazardous when combined with certain medications – gives us a clear framework for safe consumption.
Third, the data on renal function reminds us that a simple blood test can guide our decisions and prevent serious complications.
Fourth, the symptom checklist – rapid breathing, unexplained muscle cramps, sudden fatigue – acts like an early warning system, much like a smoke detector for our bodies.
Fifth, remember that not every hangover is a medical emergency, but if these red‑flag signs appear, seeking care promptly can save lives.
Sixth, the extended‑release formulation doesn’t change the lactic‑acidosis risk, but it does improve gastrointestinal tolerance, which can make adherence easier.
Seventh, staying hydrated and eating a balanced meal with your metformin dose can blunt spikes in lactate production.
Eighth, regular B12 monitoring is essential because both metformin and alcohol can deplete this vitamin, leading to neuropathy if ignored.
Ninth, keep a personal log of your drinks and any symptoms – this simple habit can help you and your healthcare team spot patterns early.
Tenth, involve your loved ones; they can remind you to stick to the guidelines and can help you get to the ER if needed.
Eleventh, if you ever anticipate a special event with heavy drinking, consider a short break from metformin – it’s a pragmatic, evidence‑based approach.
Twelfth, mental health matters too; stress can drive both alcohol misuse and poor medication adherence, so self‑care is vital.
Thirteenth, don’t hesitate to ask your doctor about alternative diabetes medications if alcohol is a regular part of your lifestyle.
Fourteenth, remember that the risk of lactic acidosis, while low, carries high mortality, so a little caution goes a long way.
Fifteenth, celebrate the small victories – a week of moderate drinking and stable glucose is a win.
Finally, stay curious, stay safe, and keep supporting each other in this journey.
Leah Ackerson
November 9, 2025 AT 23:11 PMIt’s fascinating how some folks treat a glass of wine like a badge of honor while ignoring the science 👀. The data clearly shows that binge drinking skyrockets lactic acidosis risk, yet the “I’m fine” attitude persists. Remember, a subtle symptom isn’t “just a hangover” – it can be a silent alarm. Let’s keep the conversation respectful and fact‑based, shall we? 🌟
Gary Campbell
November 11, 2025 AT 17:39 PMWhat they don’t tell you is that the pharmaceutical lobby pushes the “moderate drinking” myth to keep sales high. They hide the fact that even a single night of heavy booze can trigger MALA in vulnerable patients. Look at the suppression of independent trials that actually measure lactate spikes after alcohol – they’re buried. Trust your own body, not the glossy pamphlets.
Barbara Ventura
November 13, 2025 AT 12:08 PMWow, such a thorough post-really breaks down the risks, the symptoms, and even the practical tips, all in one place. I especially liked the checklist; having that on the fridge could be a game‑changer. Also, the bit about B12 deficiency is a nice added layer of insight, because many people overlook that connection.